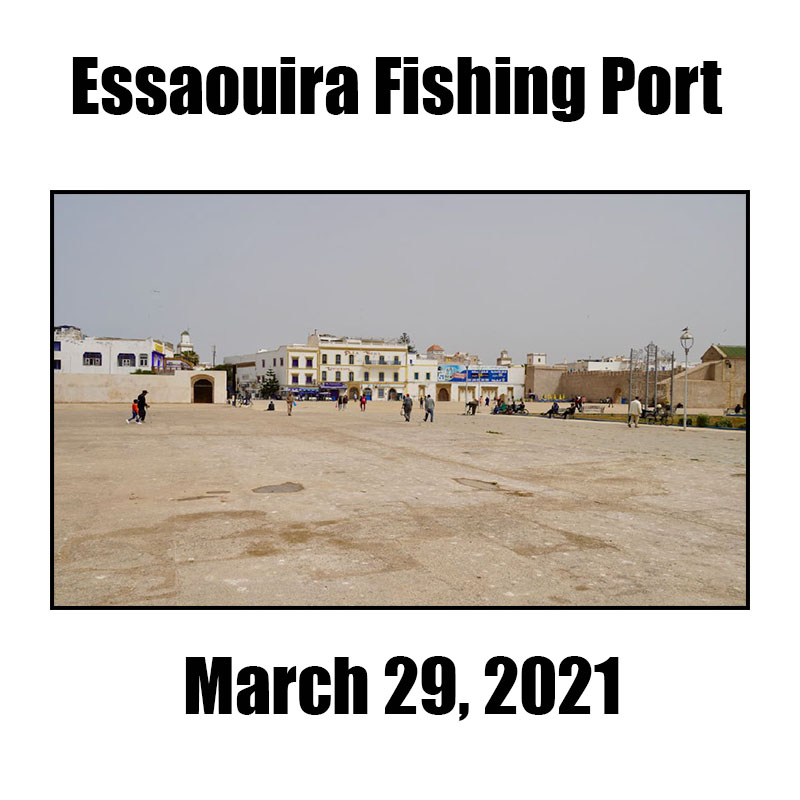
Essaouira Fishing Port – March 29, 2021 – Essaouira, Morocco
By Tom Allin
First thing I did this morning after making my morning check to confirm I was still breathing was to go to the parking lot to retrieve an item or two we had forgotten to unload yesterday. On the way back I stopped In Essaouira’s Moulay Hassan Square for a cup of coffee.
The square is huge and as you can see: empty. Essaouira has morphed from a fishing port into a tourist center during the last twenty years. However, being a year into the pandemic and Morocco still limiting Europeans and others in visiting plus the mandated closing of all restaurants at 8:00 pm has brought tourism to a standstill.
Nancy and I spent 30 minutes or more looking for the perfect café for an American egg and black coffee breakfast. When our search turned up nothing we sat down at a café, ordered eggs and coffee, and sat back to enjoy the morning.
If I didn’t have Medicare Part D, my out-of-pocket monthly expense would be about $960; Eliquis alone, without Medicare, would be $450 a month. My personal cost is about $80 a month with almost 40 percent of that amount for Eliquis alone.
Big Pharma gets away with their pricing because members of Congress are bought and paid for via campaign contributions.
Ask yourself: Why are identical drugs exponentially cheaper in other counties?
Why is a drug that costs $10 a day in Canada cost 10 times that amount in the U.S.? On average, Canadian patients pay 40 percent less than Americans.
The U.S. allows market competition to control medication pricing. This has led to higher medication prices in the U.S. than in other countries. The government in many other countries directly or indirectly manages drug costs.
The U.S. competitive marketing system, allows pharmaceutical companies to make significant profits. Manufacturers counter this complaint stating a need for profits to incentivize high-risk research.
In order for a manufacturer to get a product to market, they must pass many layers of government approval.
Between 2011 and 2015, Medicare recipients saw a 62 percent increase for brand-name drugs. The salary and pension income for those over the age of 65, however, did not meet this 62 percent rise. Thus, the steep rise in medication prices makes it very difficult for people to keep up.
Are medications really cheaper in Canada?
PharmacyChecker reports that many brand-name prescription medicines are less expensive in Canada. Yet, the U.S. Generic medications are often cheaper in the U.S. than in Canada.
Research on 20 popular brand-name drugs found a possible average savings of 70 percent when purchased in Canada. Some examples of 90-day supplies in October 2018 include:
Premarin 0.625 mg costs $623.70 in U.S. vs. $76.61 in Canada
Januvia 100 mg costs $1,593.90 in the U.S. vs. $269.94 in Canada
Crestor 10 mg costs $969.30 in the U.S. vs. $204.02 in Canada
Advair Diskus 250/50 mcg costs $1,437.99 in the U.S. vs $383.74 in Canada
Nexium 40 mg costs $863.10 in the U.S. vs. $149.94 in Canada
The U.S. government could create laws to set lower prices. Here, however, money talks and Big Pharma’s lobby
lobbyists talk BIG and LOUD!
Nothing will change until we — you, me, us, them — scream BIG and just as LOUDLY!
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.


{kind=link}
{kind=link}