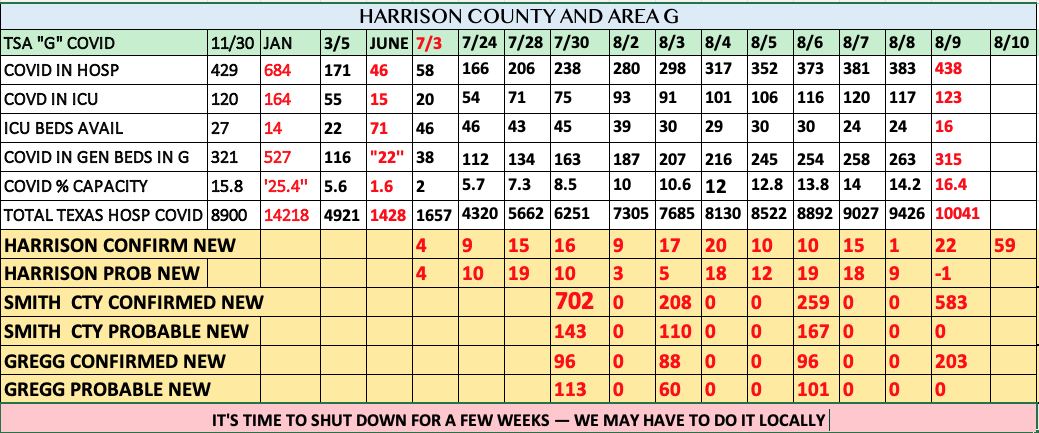
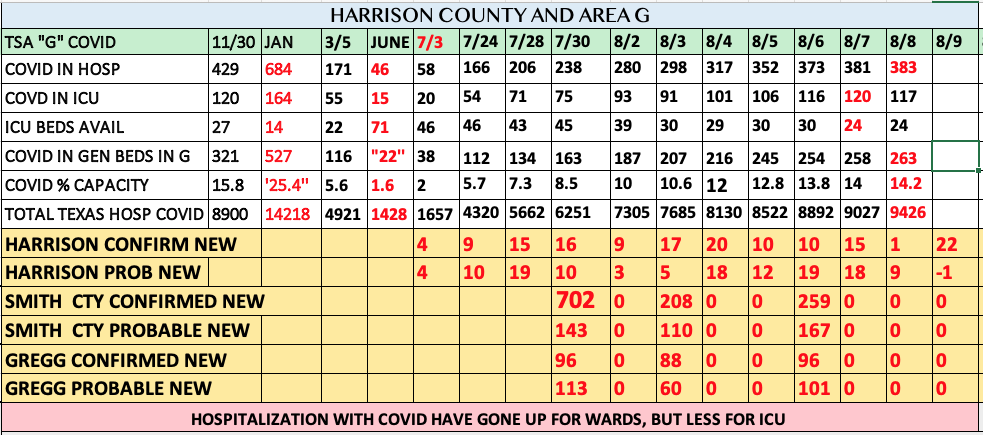
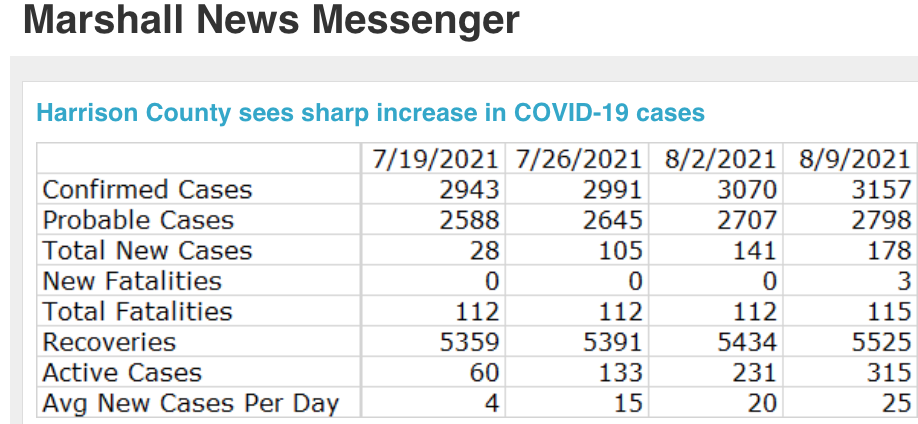
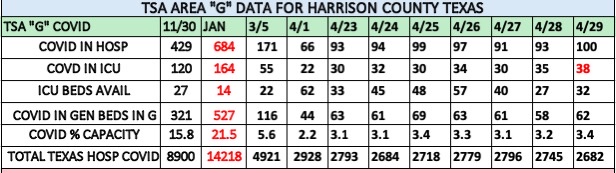
The average number of new cases in Harrison County reached 32 yesterday, a 19 percent increase from the day before. Since January of last year, at least 1 in 11 people who live in Harrison County have been infected, and at least 1 in 579 people have died.
FROM TYLER YESTERDAY:
USE OF NASAL SPRAYS AND GARGLES TO PREVENT OR ATTENUATE COVID-19 :
(J. Harris: more than you ever want to know about nose sprays and gargles)
Personal Note: My family and I use a 0.5 % nasal spray/gargle made out of 10% Betadine and our deep well water at times when area infections are rampant, before and after we go out to necessary places like the grocery store even though we also wear a mask when out. We also use it before and after being near other people, family or not, who don’t live in our house. Only recently, have we felt it prudent to use it again like we did last winter. I reviewed this topic on a mailout over a year ago and have used it intermittently ever since. So far, we have gotten away with forgetfulness when we failed to utilize it.
Does it work? I don’t know. I do think it is safe if you’re not allergic to iodine. It is said to help some people with chronic sinus infections. I feel, it’s worth a try.
I mix 5 ml of 10% Betadine Solution with 100 ml of water and distribute the mixture into a nasal spray bottle that I boiled in hot water before filling. I ordered my Betadine from Amazon, but I’m sure it’s available locally as well. It’s also cheap.
5 ml is one teaspoon (Betadine)
100 ml is about 7 tablespoons or about 3.5 oz. (water)
The resultant mixture should be about 0.5% concentration.
I think it’s safe and possibly useful. Of course, you should ask your personal physician before you try it. There are now many similar studies available that generally look good to me.
”…COVID-19 is spreading out of control in Dallas County, our North Texas region, the state of Texas and throughout much of the nation…The delta variant is truly a game changer…A forecast from UTSouthwestern Medical Center released Monday estimates that the growth rate of new cases and hospitalizations in Dallas County will continue to increase, with the county reaching more than 2,000 cases a day and 1,500-plus hospitalized patients by late August. Tripling the current pace of vaccinations would drastically lower the peak of hospitalizations the county is on track for later in the fall, the forecast found.
(Yesterday, an Internist friend of mine from Montgomery County called me to say that on Monday, he had 4 established patients, all of whom were vaccinated with two-shot vaccines, who presented to his office with symptomatic Covid infection. Two of the four were significantly ill. His patients are generally affluent and not engaged in plucking chickens or living in crowded housing. It would be interesting to know if their vaccinations were “early” like Dec. and January or later.) He’s a good doctor and they likely will do well. None of the four was hospitalized, yet).
FROM HOPKINS:
1. Safety and Immunogenicity of Heterologous Versus Homologous Prime-boost Schedules with an Adenoviral Vectored and mRNA COVID-19 Vaccine (Com-COV): A Single-blind, Randomised, Non-inferiority Trial (The Lancet) Use of heterologous prime-boost COVID-19 vaccine schedules could facilitate mass COVID-19 immunisation. However, we have previously reported that heterologous schedules incorporating an adenoviral vectored vaccine (ChAdOx1 nCoV-19, AstraZeneca; hereafter referred to as ChAd) and an mRNA vaccine (BNT162b2, Pfizer–BioNTech; hereafter referred to as BNT) at a 4-week interval are more reactogenic than homologous schedules. Here, we report the safety and immunogenicity of heterologous schedules with the ChAd and BNT vaccines.
2. SARS-CoV-2 Infection in Public School District Employees Following a District-Wide Vaccination Program — Philadelphia County, Pennsylvania, March 21–April 23, 2021 Weekly SARS-CoV-2 antigen screening tests required of all employees returning for in-school instruction in the School District of Philadelphia found a 95% lower percentage of positive test results among persons who reported receipt of 2 doses of COVID-19 mRNA vaccine (0.09%) than among those who were unvaccinated (1.77%). Efforts to promote COVID-19 vaccination among school staff members before the upcoming 2021–22 school year will be foundational to ensure a safe learning environment. (CDC MMWR, 7/30/2021)
3. COVID-19 Vaccine Safety in Adolescents Aged 12–17 Years — United States, December 14, 2020–July 16, 2021 Local and systemic reactions after vaccination with Pfizer-BioNTech vaccine were commonly reported by adolescents aged 12–17 years to US vaccine safety monitoring systems, especially after dose 2. A small proportion of these reactions are consistent with myocarditis. Mild local and systemic reactions are common among adolescents following Pfizer-BioNTech vaccine, and serious adverse events are rare. The Advisory Committee on Immunization Practices conducted a risk-benefit assessment and continues to recommend the Pfizer-BioNTech COVID-19 vaccine for all persons aged ≥12 years. (CDC MMWR, 8/6/2021)
”…There is some emerging evidence — mostly from data on adults — that Delta may cause more severe disease. Studies in Canada, Scotland and Singapore, for instance, have suggested, variously, that Delta may be more likely to lead to hospitalization, I.C.U. admission or death…Although not all states report their pediatric hospitalization rates, the data that is available suggests that they have remained essentially steady for months. Nationally, roughly 1 percent of children who are infected with the virus end up hospitalized, and 0.01 percent die, according to the A.A.P. data. Both hospitalization and death rates have declined since last summer…..It is still possible, of course, that Delta could turn out to cause more severe disease in children. Hospitalization rates, which are a lagging indicator, could rise in the weeks and months ahead. And the rare but serious inflammatory syndrome that develops in some children with Covid-19 can take weeks to appear…It is not yet clear when children under 12 may be eligible for vaccination, but in the meantime, experts said, the best way to reduce the danger to children, and relieve the stress on hospitals, is for older children and adults to get vaccinated, which will help curb Delta’s spread.”
FROM HOPKINS:
1. Antibody Development After COVID-19 Vaccination in Patients with Autoimmune Diseases in the Netherlands: a Substudy of Data from Two Prospective Cohort Studies (Lancet Rheumatology) Between April 26, 2020, and March 1, 2021, 3682 patients with rheumatic diseases, 546 patients with multiple sclerosis, and 1147 healthy controls were recruited to participate in the two prospective cohort studies. Samples were collected from patients with autoimmune diseases (n=632) and healthy controls (n=289) after their first (507 patients and 239 controls) or second (125 patients and 50 controls) COVID-19 vaccination. Among participants without previous SARS-CoV-2 infection, seroconversion after first vaccination were significantly lower in patients than in controls (210 [49%] of 432 patients vs 154 [73%] of 210 controls; adjusted odds ratio 0·33 [95% CI 0·23–0·48]; p<0·0001), mainly due to lower seroconversion in patients treated with methotrexate or anti-CD20 therapies. After the second vaccination, seroconversion exceeded 80% in all patient treatment subgroups, except among those treated with anti-CD20 therapies (three [43%] of seven patients). We observed no difference in seroconversion and IgG antibody titres between patients with a previous SARS-CoV-2 infection who had received a single vaccine dose (72 [96%] of 75 patients, median IgG titre 127 AU/mL [IQR 27–300]) and patients without a previous SARS-CoV-2 infection who had received two vaccine doses (97 [92%] of 106 patients, median IgG titre 49 AU/mL [17–134]).
2. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination — Kentucky, May–June 2021 (CDC MMWR) Among Kentucky residents infected with SARS-CoV-2 in 2020, vaccination status of those reinfected during May–June 2021 was compared with that of residents who were not reinfected. In this case-control study, being unvaccinated was associated with 2.34 times the odds of reinfection compared with being fully vaccinated. To reduce their likelihood for future infection, all eligible persons should be offered COVID-19 vaccine, even those with previous SARS-CoV-2 infection.
”…There may be something to this waning immunity story. It’s fuzzy, but the people who are getting hit are more apt to be people who were vaccinated very early…”
(J. Harris: A readable conversation between a couple of experts)
LAST BUT NOT LEASED:
THE PROBLEM WITH POLITICAL JOKES IS THAT SOME GET ELECTED
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.
If you like facts, you will want to read this article. If you don’t like facts and prefer liviing in a bubble — move on. Ron Munden
EPI UPDATE The WHO COVID-19 Dashboard reports 192.3 million cumulative cases and 4.14 million deaths worldwide as of 11:11am EDT on July 23.
Countries around the world are combating new COVID-19 surges, generally believed to be driven, in part, by increasing prevalence of the Delta variant (B.1.617.2). Unlike in previous surges, there do not appear to be strong regional trends, with the countries facing the largest surges distributed around the world. In fact, looking at the biweekly trends, there are approximately 50 countries where daily incidence has more than doubled, and they are spread across nearly every continent and region, with the notable exceptions of Central and South America.
In terms of total daily incidence, there are 15 countries reporting more than 10,000 new cases per day, including 6 reporting more than 25,000. Among these countries, 5 are in Asia (including Iran in the Eastern Mediterranean region), 4 are in Europe, 3 are in South America, and 2 are in North America. South Africa is the only African country, and none are in Oceania. Ten (10) of these countries are reporting increasing daily incidence over the past 2 weeks, including the US (+142%), Spain (+146%), and France (+287%), which more than doubled over that period. India and Argentina have exhibited decreasing trends since at least mid-June, and Brazil, Colombia, and South Africa passed their respective peaks since the beginning of July. These 16 countries account for nearly 75% of the global daily incidence. Among the countries with available data on the Delta variant, all* are exhibiting sharp increases in Delta prevalence over the past several months. India, where the variant was first reported, was first in March, and Delta prevalence began increasing in most of the other countries by late May/early June. Of the 10 countries with data available for July 12 or later, 8 are reporting higher than 70%, including 6 higher than 90%.
*Argentina does not have data available after May 17.
Similarly, the top countries in terms of per capita daily incidence represent most regions around the world. Among the top 20 countries, nearly half (9) are in Europe, 4 are in Africa, 3 are in Latin America and the Caribbean, and 3 are in Asia. Fiji is the only country in Oceania, and none are in North America. Argentina, Colombia, Malaysia, Spain, and the UK are on both lists, and considering their large populations compared to the other top per capita countries, this further illustrates the severity of their respective epidemics. All but 5 countries—Argentina, Colombia, Mongolia, Namibia, and Seychelles—are reporting increasing daily incidence over the past 2 weeks, including 9 that more than doubled over that period. Notably, Malta’s daily incidence increased nearly 1,500% over the past 2 weeks (peaking at more than 3,000% on July 16), bringing its daily average to approximately 200 new cases per day—up from 1 in mid-June. Only a small handful of these countries have data available regarding the prevalence of the Delta variant, and 4 of the 8 countries were also among the highest total daily incidence. All of these countries** reported major increases in Delta prevalence starting in May, and 5 of the 6 countries with data available for July 12 or later are reporting 80% or higher.
**With the exception of Argentina, which has no data available after May 17.
Global Vaccination
The WHO reported 3.57 billion doses of SARS-CoV-2 vaccines administered globally as of July 20. The WHO reports a total of 1.37 billion individuals have received at least 1 dose, and 656 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered fell sharply once again, now down to 29.1 million doses per day. Our World in Data estimates that there are 2.09 billion vaccinated individuals worldwide (1+ dose; 26.9% of the global population) and 1.05 billion who are fully vaccinated (13.5% of the global population).
UNITED STATES
The US CDC reported 34.2 million cumulative COVID-19 cases and 607,684 deaths. With more than 40,000 new cases per day, the US surpassed both the peak of the initial surge—31,327 on April 12, 2020—and the low reported following the summer 2020 surge—35,082 on September 13, 2020. The current average is more than 3.5 times the most recent low on June 19 (11,467) and is still increasing steadily. Daily mortality also continues to increase, up to 223 deaths per day, which is more than 40% higher than the most recent low on July 11 (159). Notably, the proportion of emergency department patients diagnosed with COVID-19 has tripled since June 21, up from 0.6% to 1.8%, which is an indication of increasing burden on health systems*.
*In an effort to provide a more accurate analysis of the current epidemiology, we are largely focusing on longer-term trends, as the most recent data are more likely to be affected by changes in the frequency of state-level reporting, particularly over the weekend.
The US CDC added a new feature to its COVID-19 Data Tracker, which displays a combination of vaccination coverage and per capita weekly incidence at the county level. The 2-dimensional coloring scheme will take some time to interpret, but it is fairly clear that the major US COVID-19 hotspots are Missouri, Arkansas, and Louisiana, where counties are reporting lower vaccination coverage and higher weekly incidence. Alabama and Mississippi are exhibiting similar trends, but to a lesser degree. Many counties in Florida are reporting elevated weekly incidence, even with higher vaccination coverage than in neighboring states. No data are available for Texas.
US Vaccination
The US has administered 340 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 446,613 doses per day*. A total of 187 million individuals in the US have received at least 1 dose, equivalent to 56.4% of the entire US population. Among adults, 68.6% have received at least 1 dose as well as 10.2 million adolescents aged 12-17 years. A total of 162 million individuals are fully vaccinated, which corresponds to 48.8% of the total population. Approximately 59.7% of adults are fully vaccinated, as well as 7.9 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current value provided here corresponds to 5 days ago.
DELTA VARIANT The US CDC continues to sound the alarm about the rapid spread of the SARS-CoV-2 Delta variant within the United States. Earlier this week, CDC Director Dr. Rochelle Walensky shared that the Delta variant now makes up 83% of domestically sequenced SARS-CoV-2 cases. This is a dramatic rise from the beginning of the month, when the Delta variant made up about half of sequenced cases within the US. There has been a corresponding rise in the number of new COVID-19 cases and related deaths throughout the month, especially impacting unvaccinated parts of the population. In a press conference earlier this week, Dr. Walensky warned that the Delta variant is one of the “most infectious respiratory viruses we know of,” urging individuals to get vaccinated. The CDC has made it clear that this will be another pivotal moment in the United States’ COVID-19 response, cautioning that many communities with low vaccination rates may face challenges of overwhelmed health care systems if preventative actions are not taken.
US CDC ACIP MEETING The US CDC’s Advisory Committee on Immunization Practices (ACIP) on July 22 concluded the benefits of the J&J-Janssen SARS-CoV-2 viral vector vaccine outweigh the risks of some people developing the rare neurological disorder Guillain-Barré syndrome (GBS) after receiving the shot. Earlier this month, the US FDA updated the J&J-Janssen vaccine’s label to warn of a possible increased risk of GBS. According to data presented at the meeting, the FDA’s Vaccine Adverse Event Reporting System (VAERS) recorded 100 preliminary reports of GBS after J&J-Janssen vaccination as of June 30, out of 12.6 million doses administered at that time. Of those cases, 95 required hospitalization, 1 person died, and 5 cases were non-serious. Dr. Hannah Rosenblum, a researcher with the CDC National Center for Immunization and Respiratory Diseases’ Division of Viral Diseases, presented data showing the risk of vaccine recipients developing GBS remained low when compared to the number of COVID-19 cases and deaths prevented by vaccination. The CDC plans to update its guidance for the J&J-Janssen vaccine to recommend that patients with a history of GBS first consider the 2-dose mRNA vaccines from Pfizer-BioNTech and Moderna, if possible. However, some panel members pointed out there are risks associated with those vaccines as well, including myocarditis and pericarditis, and that information on all of the risks associated with SARS-CoV-2 vaccines should be made available so people can make the best choice for themselves.
The ACIP also considered whether to recommend additional, or “booster,” doses of SARS-CoV-2 vaccines for people who are immunocompromised, who represent about 2.7% of the US population. Dr. Sara Oliver with the CDC National Center for Immunization and Respiratory Diseases presented data based on several small studies looking at vaccine response among immunocompromised people and additional doses in this population. Although emerging data suggest an additional SARS-CoV-2 vaccine dose in immunocompromised people enhances antibody response and increases the proportion who respond, the panel did not make an official recommendation on additional shots and will continue to review available data. Dr. Oliver also noted that serologic or cellular immune testing outside of research studies is not recommended in the US at this time. Some panel members expressed concern over immunocompromised patients getting additional vaccine doses without an official recommendation to do so, saying “the issue is almost running away from us.” Although another ACIP meeting is not yet scheduled, the panel is expected to meet again in August.
GAO PREPAREDNESS & RESPONSE REPORT The US is concurrently responding to and recovering from the COVID-19 pandemic, with an ongoing national vaccination campaign and widespread loosening of public health measures amid a recent increase in cases. Recognizing this balance as “fragile,” the US Government Accountability Office (GAO) on July 19 released its 7th comprehensive report on the COVID-19 pandemic, providing an additional 15 recommendations to various US government agencies. Previous reports included a total of 72 recommendations on COVID-19, with agencies agreeing to implement 57 of them and having fully implemented 16 to date. The most recent report makes several recommendations related to national pandemic preparedness, including advice to the CDC to develop a plan to enhance surge capacity for laboratory testing and establish contracts for the manufacturing and deployment of diagnostic test kits prior to public health emergencies. The GAO also made suggestions to the US Department of Health and Human Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) regarding the organization and oversight of the country’s Strategic National Stockpile (SNS), which provides medical supplies and other materials to respond to a broad range of emergencies. Several other recommendations relate to the oversight, timely use, and integrity of COVID-19 relief funds allocated to HHS, the US Department of Education, US Department of the Treasury, US Office of Management and Budget (OMB), and Internal Revenue Service (IRS). According to GAO, if effectively implemented, the recommendations “can help improve the government’s ongoing response and recovery efforts as well as help it to prepare for future public health emergencies.”
EXPIRING VACCINES With demand for SARS-CoV-2 vaccination largely leveling off in the US over the past 3 weeks, millions of SARS-CoV-2 vaccine doses are set to expire in the next few months. Several states and some global health experts are calling for the excess doses to be redistributed to other countries, but so far the US government has rejected those requests, citing legal and logistical challenges. However, states are now able to request a specific number of vaccine doses instead of having doses distributed to them based on their population. Delayed reporting, everyday wastage, and waning demand, including those who did not go back for second doses, are among the sources for a pile up of inventory. The FDA previously extended the shelf-life of the Pfizer-BioNTech and J&J-Janssen vaccines, and some hope an additional extension for the Pfizer-BioNTech vaccine will be approved. Meanwhile, the federal stockpile of vaccine doses continues to grow, with approximately 390 million of the 1.41 billion doses purchased by the US having been delivered, and another 562 million doses from Moderna, Pfizer-BioNTech, and J&J-Janssen expected to be delivered by the end of 2021. The White House has pledged to donate 80 million doses of its vaccine supply, and will purchase an additional 500 million doses for low- and lower-middle-income countries. But some experts note the doses currently sitting in states are ready to be administered, not waiting to be manufactured, and those doses could have a positive impact in other countries if states were permitted to redistribute them.
VACCINE MANDATES As SARS-CoV-2 vaccines become more widely available, some organizations, schools, and businesses are considering making them mandatory. This week, a US federal judge ruled to uphold a mandatory vaccination policy implemented by Indiana University, which would require SARS-CoV-2 vaccination for students, faculty, and staff before returning to campus this fall. The ruling acknowledges that the university has the authority under the Fourteenth Amendment to the US Constitution to pursue reasonable measures to protect the “public health for its students, faculty, and staff.” The students who filed the original suit are reportedly appealing the judge’s ruling.
On July 22, the American Hospital Association, the country’s largest association of hospitals and health systems, issued a statement in support of mandatory SARS-CoV-2 vaccination for healthcare workers. The statement argues that the vaccines have been demonstrated to be both safe and effective, and they play a critical role in protecting the health of both healthcare workers and their patients, many of whom are at elevated risk of severe COVID-19 disease. There have been several notable examples of hospitals firing employees who refused the vaccine, and the issue will certainly receive ongoing attention, especially until the vaccines receive full FDA approval.
VACCINE EFFICACY AGAINST VOCs A recent bioRxiv preprint study compared neutralizing antibody titers elicited by the 3 SARS-CoV-2 vaccines authorized for emergency use by the US FDA against pseudotyped variants of concern (VOCs) and variants of interest (VOIs). The small study compared blood samples from 17 people who had the 2-dose mRNA vaccines from Pfizer-BioNTech and Moderna and 10 people who received the single-dose viral vector vaccine from J&J-Janssen. Overall, the study showed a high level of antibody cross-neutralization elicited by the Pfizer-BioNTech and Moderna vaccines against VOCs but significantly decreased neutralization by antibodies generated by the J&J-Janssen vaccine. Because the study was conducted using blood samples, it might not reflect real-world performance, but the results counter previous reports of the J&J-Janssen vaccine’s efficacy against the Delta variant. The authors of the bioRxiv study, which is not yet peer-reviewed, said they hoped the findings did not discourage people from getting the J&J-Janssen vaccine but that future recommendations included advice for an additional second dose of that vaccine or an mRNA vaccine. The authors also called for continued surveillance of breakthrough infections to help determine the real-world effectiveness of the vaccines.
Another study evaluating vaccine effectiveness against the Delta variant was published July 21 in the New England Journal of Medicine. This study compared the effectiveness of the Pfizer-BioNTech mRNA vaccine and AstraZeneca-Oxford viral vector vaccine against the Alpha and Delta variants. Following 1 dose of the 2-dose vaccines, effectiveness was notably lower among persons with the Delta variant (30.7%) than among those with the Alpha variant (48.7%), with the results similar for both vaccines. Following a second dose, the Pfizer-BioNTech vaccine was 93.7% effective against Alpha and 88% effective against Delta. The AstraZeneca-Oxford vaccine after 2 doses was 74.5% effective against Alpha and 67% against Delta. The researchers note the differences in effectiveness between the vaccines are considered modest and support public health efforts to maximize uptake of the full 2-dose regimen to protect against VOCs.
REAL-WORLD VACCINE EFFECTIVENESS A study published July 20 in the Annals of Internal Medicine details a test-negative case-control study examining the short-term effectiveness of authorized SARS-CoV-2 mRNA vaccines in preventing infections. The research team used data collected through the US Department of Veteran Affairs’ (VA) COVID-19 Shared Data Resource, a national database containing extensive demographic, clinical, pharmacologic, laboratory, vital sign, and clinical outcome information derived from multiple validated sources. The researchers identified all individuals who tested positive for SARS-CoV-2 infection between December 15, 2020 and March 4, 2021, and matched them with control participants who had similar factors such as sex, age, race, BMI, and geographic location, but who had tested negative for SARS-CoV-2. The main measure of interest was vaccine effectiveness 7+ days after the second vaccine dose, but the researchers also examined vaccine effectiveness among those who received only 1 dose of either the Pfizer-BioNTech or Moderna vaccines.
The team identified 54,360 matched pairs of veterans. Among those who tested positive, 18% had been vaccinated, compared with 32.8% of those who tested negative. Overall, the vaccines showed 97.1% effectiveness among those who received the second dose at least 7 days prior. Among those who received only 1 dose, effectiveness was 85% overall. The research team concluded the SARS-CoV-2 vaccines being employed by the VA provided a high level of protection against infection. However, they noted several limitations of the study, including a predominantly male study population, a lack of data for currently circulating SARS-CoV-2 variants of concern, and a short follow-up period.
HEALTH EFFECTS OF LOCKDOWNS Researchers continue to explore the potential unintentional health impacts of COVID-19-related lockdowns. A commentary
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.
‘The U.S. Government [is] pouring more than $3 billion on a neglected area of research: developing pills to fight the virus early in the course of infection, potentially saving many lives in the years to come….A number of other viruses, including influenza, H.I.V. and hepatitis C, can be treated with a simple pill. But despite more than a year of research, no such pill exists to treat someone with a coronavirus infection before it wreaks havoc.”
(J. Harris: These “antibiotics” can and will be developed.)
(J. Harris: From AP is easy to understand format. I’m not sure just what it means, yet.)
FROM HOPKINS CITATIONS:
1. Monoclonal Antibodies Cut Risk of Dying from COVID-19—But Only in Some Patients (Science)The world’s largest trial of COVID-19 therapeutics has for the first time produced convincing evidence that a therapy that directly attacks the virus can save hospitalized patients from death. A combination of antibodies called casirivimab and imdevimab, produced by Regeneron, did not lower mortality when all patients in the study were taken together, investigators of the United Kingdom’s Recovery trial announced today—but it reduced deaths by one-fifth among those who did not produce antibodies themselves. A paper with the results will be made available on the medRxiv preprint server later today, the researchers say.
2. Many Post-Covid Patients Are Experiencing New Medical Problems, Study Finds (New York Times) Hundreds of thousands of Americans have sought medical care for post-Covid health problems that they had not been diagnosed with before becoming infected with the coronavirus, according to the largest study to date of long-term symptoms in Covid-19 patients.
FROM BECKERS( they closely follow CDC and many other journals and do nice, succinct reviews which are amazingly pertinent — and you can have them sent directly to you.)
Among patients hospitalized with Covid-19 pneumonia, tofacitinib led to a lower risk of death or respiratory failure through day 28 than placebo….”
(J. Harris — THIS IS A LETHAL PNEUMONIA: “A total of 289 patients underwent randomization at 15 sites in Brazil. Overall, 89.3% of the patients received glucocorticoids [as well as Tofacitinib or Placebo] during hospitalization. The cumulative incidence of death or respiratory failure through day 28 was 18.1% in the tofacitinib group and 29.0% in the placebo group…”)
Vaccine breakthrough cases are expected. COVID-19 vaccines are effective and are a critical tool to bring the pandemic under control. However, no vaccines are 100% effective at preventing illness in vaccinated people. There will be a small percentage of fully vaccinated people who still get sick, are hospitalized, or die from COVID-19.
More than 139 million people in the United States have been fully vaccinated as of June 7, 2021. Like with other vaccines, vaccine breakthrough cases will occur, even though the vaccines are working as expected. Asymptomatic infections among vaccinated people will also occur.
There is some evidence that vaccination may make illness less severe for those who are vaccinated and still get sick.
Current data suggest that COVID-19 vaccines authorized for use in the United States offer protection against most SARS-CoV-2 variants currently circulating in the United States. However, variants will cause some vaccine breakthrough cases.
(J. Harris: The new vaccine (NOVAVAX) might be effective in immunocompromised patients.)
FROM HOPKINS
1. PRESS RELEASE
HHS Awards $125 Million in Workforce Grants for Community-Based Efforts to Bolster COVID-19 Vaccinations in Underserved Communities The US Department of Health and Human Services, through the Health Resources and Services Administration (HRSA) awarded $125 million to support 14 nonprofit private or public organizations to reach underserved communities in all 50 states plus the District of Columbia, Puerto Rico, Guam and the Freely Associated States to develop and support a community-based workforce that will engage in locally tailored efforts to build vaccine confidence and bolster COVID-19 vaccinations in underserved communities. These awards reflect the first of two funding opportunities announced by President Biden last month for community-based efforts to hire and mobilize community outreach workers, community health workers, social support specialists, and others to increase vaccine access for the hardest-hit and highest-risk communities through high-touch, on-the-ground outreach to educate and assist individuals in getting the information they need about vaccinations.
(J. Harris: Do we have someone working on this????)
2. DELTA VARIANT As countries around the world continue to expand vaccination efforts, there is growing concern that the Delta variant of concern (B.1.617.2; VOC) could cause significant problems before many countries can achieve sufficient vaccination coverage. The Delta variant is the most recent VOC designated by the WHO and US CDC. Reportedly, the current COVID-19 surge in southeastern China is being driven by the Delta variant, and other countries are adapting COVID-19 restrictions in order to mitigate the risk from this VOC. Emerging evidence indicates that the Delta variant poses an elevated risk for severe disease compared to others, and it is believed that the variant is largely responsible for India’s largest surge, which peaked in early May. The Delta variant also represents an increasing proportion of COVID-19 cases in the US—up to 6%, compared to 1% only a month ago—and the UK at 91% of new cases. In response to increasing prevalence of the Delta variant, the UK is extending existing COVID-19 restrictions for another 4 weeks—shifting the expected date from June 21 to July 19—which will allow for accelerated vaccination efforts before taking further steps to ease restrictions.
Emerging data indicate that existing vaccines, including the Pfizer-BioNTech and AstraZeneca-Oxford vaccines, are effective in preventing severe disease and hospitalization….”
“In summary, we show that the Delta VOC in Scotland was found mainly in younger, more affluent groups. Risk of COVID-19 hospital admission was approximately doubled in those with the Delta VOC when compared to the Alpha VOC, with risk of admission particularly increased in those with five or more relevant comorbidities. Both the Oxford–AstraZeneca and Pfizer–BioNTech COVID-19 vaccines were effective in reducing the risk of SARS-CoV-2 infection and COVID-19 hospitalisation in people with the Delta VOC, but these effects on infection appeared to be diminished when compared to those with the Alpha VOC. We had insufficient numbers of hospital admissions to compare between vaccines in this respect. The Oxford–AstraZeneca vaccine appeared less effective than the Pfizer–BioNTech vaccine in preventing SARS-CoV-2 infection in those with the Delta VOC. Given the observational nature of these data, estimates of vaccine effectiveness need to be interpreted with caution.
(J. Harris: Delta makes young people sick, sometimes very sick. Vaccines worked in prevention, but it took a month to get protected: “Overall, a strong vaccine effect did not clearly manifest until at least 28 days after the first vaccine dose…”
THE EPIDEMICS IN MARSHALL. (From old notes from newspapers)
Gladys Knight:
The greatest epidemic Marshall has ever had is the one recorded in a little paper, “The Marshall Sentinel”, published in 1873. This epidemic was the yellow fever. From the “Iron Age Extra” October 30 we find that “a quarantine be raised between Shreveport and Marshall so far as the freight of all description, but be continued as to the citizens of Shreveport.” They also advised that “citizens absent from this place remain absent until further notice”. From September 10th to October 30th, 1873, there were seventy deaths from yellow fever.
In 1900 Marshall had an epidemic of Small Pox.
Later in 1912 there was an epidemic of meningitis. There was no record kept of the number of cases or deaths during this dreaded epidemic, but we know that there were many cases; a few of these proved fatal. (Could this have been an Equine Encephalitis instead?)
The next epidemic that Marshall had was in 1918 and early part of 1919. This epidemic was the Influenza which is commonly known as the “Flu”. There were between six hundred and seven hundred cases in Marshall, only seventy of which proved fatal.”
(J. Harris: One case report — successful treatment.)
From the Washington Post:
A dispute over vaccination status is taking place in a South Dakota courtroom, where a federal judge has filed criminal contempt charges against three members of the U.S. Marshals Service. U.S. District Judge Charles Kornmann asked the three marshals whether they were vaccinated, and when a deputy marshal refused to answer, the judge ordered her out of the courtroom. The other marshals left, too, taking defendants with them. In a letter, the judge said he expects to know the vaccination status of people working in the courtroom as a matter of “protecting all of us who serve the public.”
(J. Harris: SD is always exciting)
AND LAST BUT NOT LEASED:
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.
During the second wave of the COVID-19 pandemic in India, which began in March, 2021, demand on the health-care system has far exceeded capacity. Despite crippling shortages, patients are prescribed a battery of ineffective therapeutic interventions.1 Ivermectin, hydroxychloroquine, and herbal cocktails continue to receive state patronage.2, 3, 4 On May 8, 2021, 2-deoxy-D-glucose was given emergency authorisation, stating that it will “save precious lives” without any published evidence that it impacts mortality.5 An entrenched culture of polypharmacy and gestalt-driven practice among physicians has resulted in indiscriminate and unwarranted use of remdesivir, favipiravir, azithromycin, doxycycline, plasma therapy, and most recently baricitanib and bevacizumab, regardless of disease severity or drug efficacy. Excessive and inappropriate use of steroids could be contributing to the alarming rise of mucormycosis in patients recovering from COVID-19.
In rural India, where health-care infrastructure is threadbare, and families are poor, patients can ill afford such expensive mistakes. Honing in on the most high yield and affordable interventions, we propose recommendations for testing and management, optimised to India’s current resource-constrained context (table). Every clinical touchpoint should be used to underscore masking, distancing, and vaccination.
“….Alpha’s ability to outstrip previously circulating variants could stem from mutations in its spike protein that allow it to enter cells more efficiently… Alpha also has tricks linked to mutations outside the spike protein. These mutations probably mean that within hours of infecting a person, Alpha suppresses the rapid-response defence that the body mounts against all invaders. By blocking this ‘innate immune response [interferon]’, the virus buys itself more opportunities to infect other people….cells from the human airway produced interferon, an immune protein that kick-starts the body’s defences on the arrival of a pathogen. The team found that cells infected with Alpha produce much less interferon than do cells infected with previously circulating SARS-CoV-2 variants. Alpha’s suppression of interferon production helps the variant to stick around for longer in the body.
…The team attributes this over-expression to a mutation outside the spike protein, in genes that are important for viral replication. The latest paper “highlights the importance of looking beyond the spike protein for new mutations…”
FROM HOPKINS CITATIONS”
1. The mRNA Vaccine Revolution is Just Beginning (WIRED) The scope of mRNA vaccines always went beyond any one disease. Like moving from a vacuum tube to a microchip, the technology promises to perform the same task as traditional vaccines, but exponentially faster, and for a fraction of the cost. “You can have an idea in the morning, and a vaccine prototype by evening. The speed is amazing,” says Daniel Anderson, an mRNA therapy researcher at MIT. Before the pandemic, charities including the Bill & Melinda Gates Foundation and the Coalition for Epidemic Preparedness Innovations (CEPI) hoped to turn mRNA on deadly diseases that the pharmaceutical industry has largely ignored, such as dengue or Lassa fever, while industry saw a chance to speed up the quest for long-held scientific dreams: an improved flu shot, or the first effective HIV vaccine.
FROM THE ATLANTIC:
What we know about Delta, the new coronavirus variant:
“…It’s more dangerous to be unvaccinated now than it was to be unvaccinated this time a year ago. We know the virus is changing in ways that make it more dangerous. And so if you encounter the virus now, you’re encountering a more problematic pathogen…The U.K. is delaying its reopening because of Delta..
[but] given the trajectory we’ve been on for the past several weeks, shutdowns like last spring’s may not be necessary. But we can’t completely forecast things such as how the virus is going to change…we never had a national lockdown in the U.S. throughout this entire thing. And now that the vaccines are here, we have this incredibly powerful weapon. Keeping vaccination rates high and sharing our vaccines with the world could be a way to further ensure that the U.S. doesn’t need to turn to lockdowns at all…[ther is] a lot of optimism from experts in recent weeks. [some experts think] if we haven’t fully turned a corner in this country, we’re in the process right now…It’s not like we’re going to reach utopia by October. But we still have more vaccines in the pipeline.
(J. Harris: Good. They deserved it. Their fabulous writers surround, explore, and prod problems and then disseminate information better than any news, social, or governmental organization of which I am aware. If I could only read one “thing” daily, it would be the Times. I rarely read their editorials; I love their sports department, which for over ten years has been hammering away at Chronic Traumatic Encephalopathy (CTE) and for which they deserve another Pulitzer Since early 2020, this paper has provided the best Covid-19 coverage that I have found. Over about the last six months, they have become so adept that they save me an hour or two on most days while I try to keep up with the local ramifications of the Pandemic. CONGRATULATIONS NEW YORK TIMES.
FROM HOPKINS CITATIONS:
1. Mixing COVID-19 Vaccines Appears to Boost Immune Responses (Science) Faced with short supplies of COVID-19 vaccines and unforeseen side effects, some countries have adopted an unproven strategy: switching shots midstream. Most authorized vaccines require two doses administered weeks or months apart, but Canada and several European countries are now recommending a different vaccine for the second dose in some patients. Early data suggest the approach, born of necessity, may actually be beneficial.
2.No Health Issues in Babies Whose Moms Got Flu Vaccine While Pregnant (CIDRAP) Infants who were exposed to the flu vaccine in utero—meaning their mothers received the vaccine while pregnant—did not have an increased likelihood of adverse outcomes, according to a study today in JAMA. The study looked at more than 99% of live births during the 2010-11 to 2013-14 flu seasons in Nova Scotia, Canada.
Our estimation of 51% vaccine effectiveness against PCR-confirmed SARS-CoV-2 infection and 54% vaccine effectiveness against symptomatic infection 13 to 24 days after immunization with first dose of BNT162b2 provides critically needed evidence on the early performance of BNT162b2 vaccine in real life and has some important implications in decision-making to prevent transmission of SARS-CoV-2 and control the pandemic. While these results are encouraging, the BNT162b2 vaccine should be administered in a 2-dose regimen 21 days apart, as licensed for emergency use approval, to achieve maximum protection and impact in reducing the burden of COVID-19 and possibly the transmission of SARS-CoV-2.
(J. Harris: A study from Israel shows TAKE BOTH JABS!)
(J. Harris: Good general and readable article to send to the unvaccinated wary.)
AND LAST BUT NOT LEASED:
My Norwegian Housekeeper is back to work with her new hip. Here she is helping in the garden.
Maybe she’ll be cooking again soon?
As far as the garden in concerned, I’ve not had to water in a month. Unfortunately, some of the tomatoes that I planted early and surrounded by old newspapers, developed non-venereal root rot. The leaves yellowed and died, the stems turned black and dreary and the tomatoes quit growing. I cut off the bad leaves and removed the newspapers to let things dry out. I was not surprised when I noticed that all of the sick plants had been covered by Longview News.The plants protected by Marshall News Messengerwere in semi-perfect. condition! Strangely, a couple of plants on the far left side of the garden that were covered by New York Times, must have caught on fire and were charred. I don’t know what all of this means, and I was a scientist or sorts. I kid you not. J. Harris
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.
(J. Harris: Good short summary from Washington Post; we looked at some of this earlier)
“Britain has fully vaccinated more than 41 percent of its population, while more than 60 percent have received at least one shot. But over recent weeks, the number of new cases recorded daily has ticked slowly but surely up, while health authorities confirmed last week the delta variant had come to dominate new infections.What we know about the highly infectious coronavirus delta variant includes…Also known by the scientific name B.1.617, the variant was first identified in Maharashtra, India, in October…Though it is just one of many variants to have arisen during the pandemic, it is considered one of the most alarming… the British government believed that the delta variant was 40 percent more transmissible than the alpha variant, also known as B.1.1.7, which was first detected in Britain…the majority of new cases in the country are among those not yet vaccinated. Nearly all serious cases have been recorded among the unvaccinated or partially vaccinated..The jabs are working…We have to keep coming forward to get them, and that includes vitally that second jab, which we know gives better protection against the delta variant…Relaxation of public health and social measures, increased social mobility, virus variants and inequitable vaccination are a very dangerous combination,” (J. Harris: and the US is at risk.)
FROM HOPKINS CITATIONS:
1. Last week, researchers reported in The Lancet that the Pfizer-BioNTech SARS-CoV-2 vaccine elicited a weaker antibody response to the delta variant than to the original wildtype virus, especially among older populations. The data raise the likelihood of a booster shot being needed for some people, although the scientists cautioned that more data are needed to know whether the vaccine would be any less effective at preventing severe disease, hospitalization, or death
(J. Harris: The article is unreadable for me; the new Greek alphabet designations were not yet selected for the variants. A booster might be necessary to prevent Delta especially in old, fat people who took the Pfizer vaccine. Uh Oh.)
2. Drop in Convalescent Plasma Use at U.S. Hospitals Linked to Higher COVID-19 Mortality Rate (JHSPH) A new study from researchers at Johns Hopkins Bloomberg School of Public Health and colleagues suggests a slowdown in the use of convalescent plasma to treat hospitalized COVID-19 patients led to a higher COVID-19 mortality during a critical period during this past winter’s surge.
3.China is Vaccinating a Staggering 20 million People a Day (Nature) For more than a week, an average of about 20 million people have been vaccinated against COVID-19 every day in China. At this rate, the nation would have fully vaccinated the entire UK population in little more than six days. China now accounts for more than half of the 35 million or so people around the world receiving a COVID-19 shot each day.
In an interview with the state broadcaster China Central Television, Sinovac’s chairman, Yin Weidong, said the company’s clinical trials involving “hundreds” of people had found that its vaccine was just as safe and effective in people ages 3 to 17 as it was in adults.
(J. Harris: Fortunately, there is little need for the US to be in a hurry with this age group at this time.)
“…Experts say the exact reason behind this trend is unclear, but could include the rise of variants, relaxed attitudes towards distancing and other mitigation measures, a younger population that is not yet fully vaccinated and vaccine hesitancy. It could also be merely more younger people getting the disease…There is a very sharp increase…in younger adults… these are largely people who think that their age is protecting them from getting very sick from COVID-19, that is not happening…40% of our cases were under the age of 40, which is mind-boggling…Hospitals are seeing more and more younger adults, those in their 30s and 40s, admitted with severe disease,” Centers for Disease Control and Prevention (CDC) Director Dr. Rochelle Walensky reported during a press briefing earlier this month.
(J. Harris: Excellent article for Long Haulers and their families detailing the frequency of various long term health problems after Covid).
HOPKINS CITED:
1. Merck Announces Voluntary Licensing Agreements With Five Indian Generics Manufacturers to Boost Access to COVID-19 Therapeutic (Homeland Preparedness News) Merck has reached voluntary licensing agreements with five Indian generics manufacturers to produce molnupiravir for the COVID-stricken nation, granting it another oral therapeutic to aid the COVID-19 pandemic. While molnupiravir is currently being studied in a phase three trial to treat non-hospitalized patients with COVID-19, these agreements will allow Merck to accelerate the availability of the therapeutic in India and other low and middle-income countries following approvals or emergency authorization by regulatory agencies. Some vaccinated people are still getting covid. Here’s why you shouldn’t worry. (MIT Tech Review) Tens of millions of people in the United States have now been fully vaccinated against covid-19. These people are seeing friends, eating out, and—in rare cases—getting infected.
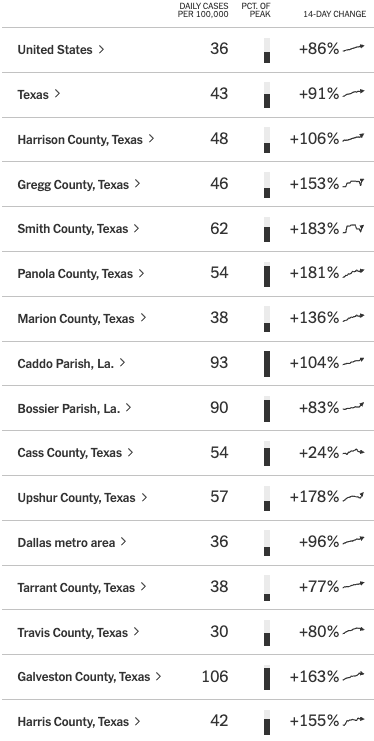
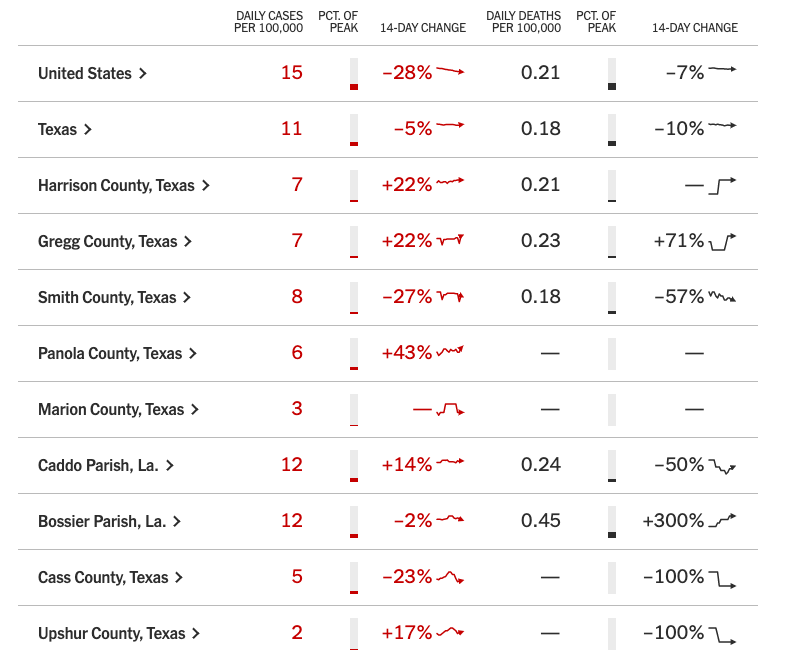
J. Harris: What I like about this NYT Tracker Chart is that it comes daily and compares the disease incidences in area counties as well as the state, US, and world with “Daily Cases Per 100,000 [population].” There are fewer man-made distortions in the numbers. They are also a tremendous time-saver. You can also make your own tracker and keep up with areas of personal interest.
AND LAST BUT NOT LEASED:
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.
So-are-we-never-going-to-learn headline of the day
By George Smith
“Chris Christie Gives One-Term, Twice-Impeached Trump An ‘A’ For His Presidency”
This is the same former New Jersey governor who said Trump was double-dog-dead-ass wrong in contesting the 2020 election. This is the same guy who called the president’s legal team a “national embarrassment”.
Chris Christie has already set his sights on running for president, even if Trump decides to run; he is sacrificing his soul by trying to buddy-up to the Trumpuppet Clan.
The most prominent Republicans, those that think they can lead the party out of its self-ordained quagmire, are four-square pitiful and are embarrassing themselves by constantly rubbing Trump’s belly for luck.
Trump ain’t Buddha. He’s Trump. And it should be clear by now that all those around him, all those that rush to bask in his aura, all who will do whatever it takes to win support from his Clan of Cultish Clowns…are doomed to be sucked into history’s vacuum and forever labeled as pathetic, corrupt, unAmerican losers.
The story of the era of Trump is already written. And more indictments of this era of political tomfoolery and folderol are being immortalized by today’s vaunted historians right now.
Doris Ketns Goodwin, Jon Meacham, Michael Beschloss and Robert McDonald will dissect Trump’s president “seven ways to Sunday,” as my grandfather used to say.
And those that supported the man, his vitriolic mission, his cartoon-car of idiotic ideas, his racist agenda, his tarnishing of the title he had, the prestige he enjoyed by his election…they are complicit in the corruption that ensued and the division that resulted from his and his party’s actions.
As a country, we will survive and thrive again. And every American should pray that we learned a valuable lesson over the last four years and pledge never to put our faith in a corrupt, ignorant, bumbling heretic again.
***********************************
GIVE US YOUR FEEDBACK. CLICK ON “COMMENT” TO TELL US WHAT YOU THINK or use one of the alternative methods for providing feedback.


























{kind=link}
{kind=link}